MEDICATED ASSISTED THERAPY
Medicated Assisted Therapy
Opioids boost dopamine levels by stimulating molecules called mu opioid receptors that sit on the surface of certain neurons. Normally, these receptors are activated by hormones and brain chemicals made in the body, such as endorphins (endogenous opioids), to reinforce pleasurable behavior such as eating, having sex or listening to music. A single dose of heroin releases many times the amount of dopamine that is produced by a favorite food or song.
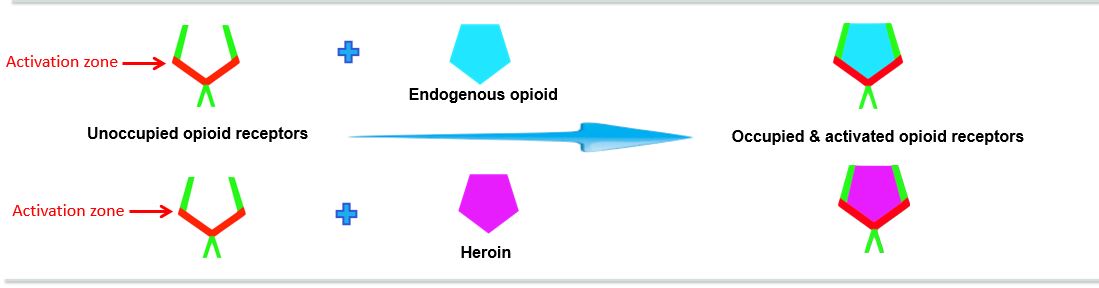
There are different types of medication used for heroin/opioid addiction recovery. All bind to the opioid receptor but have different effects.
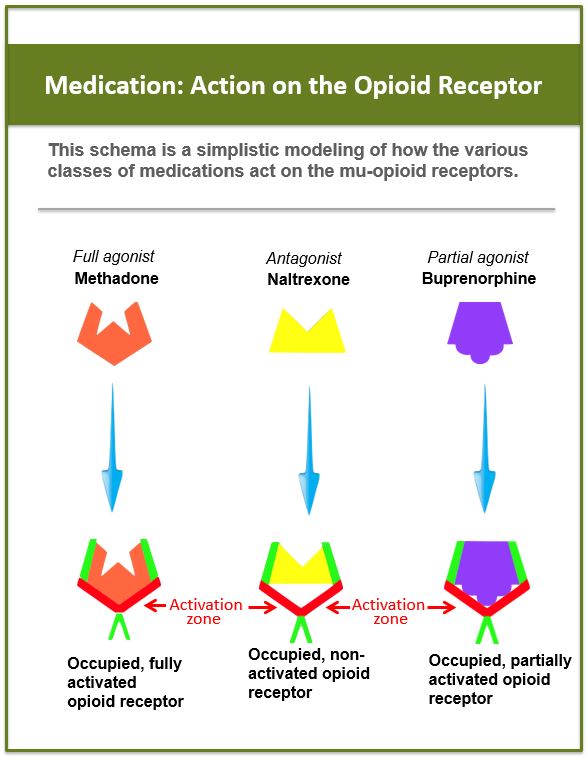
Methadone
FULL AGONIST
Like heroin, methadone fully occupies and activates the mu opioid receptor (see box on the right). However, there are significant differences between heroin and methadone, for example: heroin gives a peak “rush” and has a fairly rapid metabolism (4-5 hours) resulting in extreme highs and lows. Methadone occupies the mu-opioid receptors without offering an initial “rush” and is metabolized very slowly, up to 36 hours. This allows for a stabilization of the patient seeking recovery from heroin addiction because, a) the opioid receptors are occupied so heroin, if introduced, would not have a receptor to bind to and, b) because the receptors are activated at a consistent level, the person suffering from opioid addiction can resume normal functioning without withdrawal symptoms or the intense craving for heroin. Methadone is a full agonist because it occupies and fully activates the receptor (see box).
Naltrexone, Naloxone
ANTAGONISTS
Antagonists occupy the mu opioid receptor but do not activate it (see box on right). Because they occupy the same receptors as opioids seeks, if the person recovering from opioid addiction uses heroin/opioids, the opioids have no receptors to bind to, thus, the individual does not get the sought for “reward.” Antagonist medications include naltrexone, vivitrol, nalmefene and naloxone. Naloxone is short-acting and, therefore, is not used in MAT (except as noted below, “Suboxone: what is it?”). Naltrexone can be administered via daily tablets, monthly injections (vivitrol), and implants, whose effects last up to 6 months.
Buprenorphine
PARTIAL AGONIST
The buprenorphine based medications such as Suboxone and Subutex used in MAT are partial agonists (see box on right). Since buprenorphine partially activates the opioid receptor, it helps to reduce intense heroin/opioid cravings; and because it occupies the same receptors as heroin seeks, if heroin/opioids are used, they have no receptors to bind to and the sought for “reward” is not achieved.
Want to know more about how Suboxone works? See below.
SUBOXONE: what is it?
Suboxone is a mixture of buprenorphine and Naloxone. Naloxone is added to discourage misuse of buprenorphine during recovery from opioid addiction.
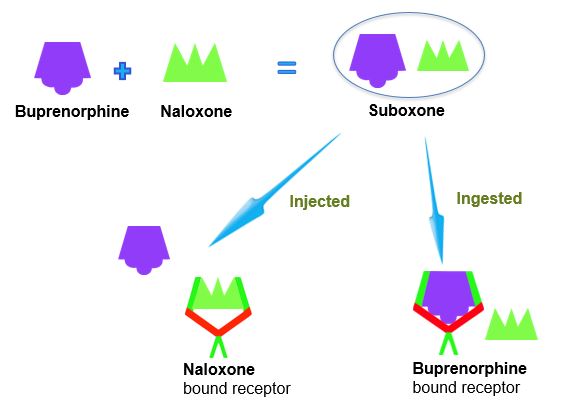
The active ingredient in Suboxone is the partial agonist, buprenorphine. However, it also contains the antagonist drug naloxone (Narcan). Naloxone is added for the sole purpose of reducing the incidence of abuse. When suboxone is taken as prescribed (by mouth), the buprenorphine will reach the opioid receptors first and naloxone will not be able to displace it because buprenorphine binds tightly to the opioid receptor. However, if the patient attempts to inject the suboxone hoping for buprenorphine “high,” the naloxone will more immediately occupy the receptors, blocking the buprenorphine effects.
Buprenorphine bound receptors are stable in the presence of naloxone (Narcan) and other opioids such as heroin.
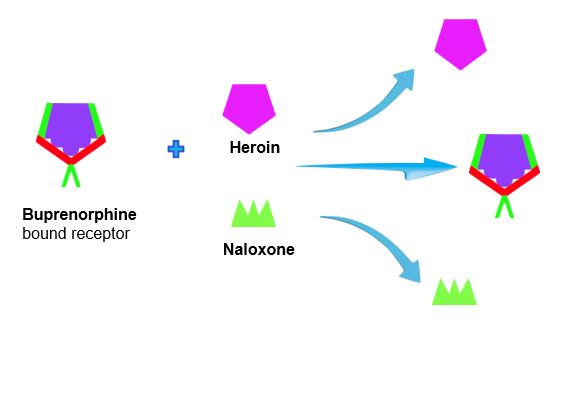
Buprenorphine sits snugly in the opioid receptor and partially stimulates it. For this reason, it is considered a partial agonist. Neither morphine (heroin) nor naloxone (Narcan) can displace buprenorphine from the receptor once it is bound. Therefore, heroin/opioids, if used when buprenorphine is bound, will not give the desired effect to the patient. Important to note, though buprenorphine overdose is rare, naloxone will likely not reverse a buprenorphine overdose.
NALOXONE: what is it?
Reversing an Overdose
Naloxone has a high affinity for the opioid receptor
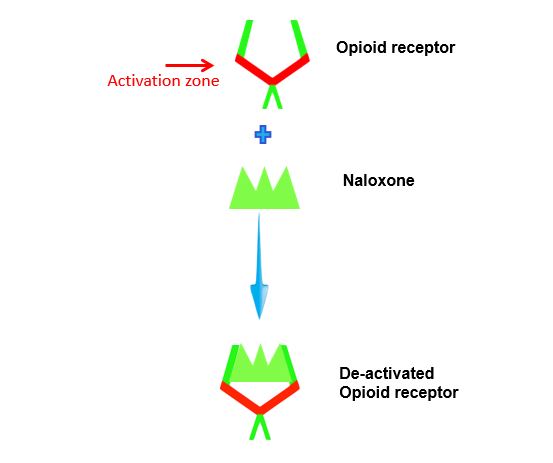
Like naltrexone, naloxone binds to the opioid receptor and does not activate it. It also prevents other opioids from binding to the receptor. However, since it is short-acting, it is not used in medicated assisted therapy except as a barrier to the abuse of buprenorphine in Suboxone (as explained above). However, because of its high affinity for the opioid receptor it is effective in reversing an opioid overdose.
Naloxone is used to reverse an opioid overdose by displacing the opioid from the opioid receptor.
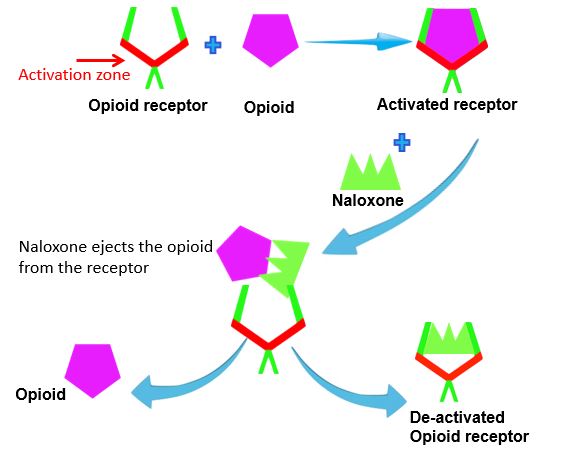
When naloxone is introduced to an opioid-bound receptor, it will kick the opioid out of the receptor because it has a higher affinity for the receptor. It does not stimulate the receptor because it does not sit in the activation zone, therefore, it is considered to be an opioid antagonist.
FOR MORE INFORMATION
LATEST NEWS

Truth Pharm rallies at Elmira State Prison
Dozens of protesters chanted outside the Elmira Correctional Facility Tuesday morning, calling for...

Truth Pharm Supports the End Overdose NY Campaign in Albany
On Monday, 1/29/18 NINE Rainmakers headed to Albany to advocate for the #EndOverdoseNY Campaign....

Drive For Change
Truth Pharm is pleased to announce it’s first annual Drive For Change golf tournament! Along with...
LOCATIONS
East Coast
- Southern Tier
- Southern Chenango County Recovery Resources
- Sherburne-Earlville
West Coast
- Los Angeles
CONTACT
Truth Pharm, Inc
PO Box 424
Binghamton, NY 13902
49 Pine St. Suite 6
Binghamton, NY 13901
607-296-3016
info@TruthPharm.org